Basic HTML Version



or infection and may expedite a return to the water. Learn more about
your ears and how to take care of them with DAN’s online seminar “Ears
and Diving,” available at www.DAN.org.
Q:
Last fall I underwent a pulmonary vein ablation for atrial
fibrillation. Five months later my cardiologist ordered an
echocardiogram with bubble study to confirm closure of the
puncture in my interatrial septum. Unfortunately, the hole persists.
The cardiologist admitted to an incomplete understanding of the
relevant issues but recommended I refrain from diving until closure
of the hole can be confirmed or it is surgically repaired. What can
you tell me about my fitness to dive?
A:
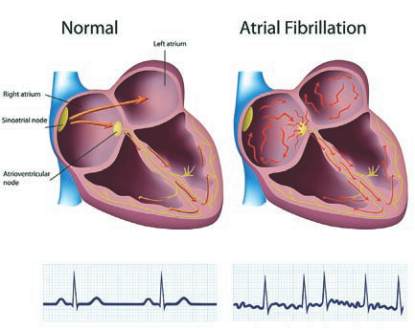
Atrial fibrillation (a-fib) is one of the most common rhythm
disorders encountered in clinical cardiology. Basically, the atria
(upper chambers of the heart) quiver rather than contracting in
an organized fashion. This leads to a very rapid and irregular heart rhythm
that can be quite uncomfortable (though some people do not experience
symptoms) and may put patients at a significantly increased risk for stroke.
Risk factors for the development of a-fib are hypertension, underlying
coronary artery disease, increasing age and valvular heart disease.
In the past, the intention of therapy was to either slow the rate of
the fibrillation (using drugs or catheter-based radiofrequency ablation)
or control the rhythm with drugs. Success rates at maintaining normal
rhythm over the next year were generally less than 50 to 70 percent.
Atrial fibrillation can now be treated in selected patients with catheter-
based isolation of the pulmonary veins in the left atrium. This procedure
has a long-term success rate of about 80 percent, but it requires the
cardiologist to puncture the interatrial septum to get from the right atrium
to the left atrium. The hole or holes usually close spontaneously over time,
but they don’t always. Until they are closed the patient is left with an atrial
septal defect of sorts — similar to a congenital “hole in the heart.” This
means venous bubbles might bypass the lungs (which act as bubble filters)
and cross into arterial circulation. This would put a diver at an increased
risk of decompression illness (DCI). Information is limited, but the increase
in risk seems to be about fivefold and is likely related to the size of the hole
or holes. Although that may sound like a dramatic increase, the risk of DCI
in recreational diving is about 2 per 10,000 dives. Thus, a fivefold increase
in this risk is only 1 per 1,000 dives — still a very low absolute risk.
52
|
SUMMER 2012
Meets 2010
ILCOR/AHA Guidelines
Find a DAN Instructor
in your area today!
Search the online directory
of DAN Instructors
www.DAN.org/training/directory
or call DAN Education at
919-684-2948, ext.555
Be a
Prepared Diver
Take DAN’s newly revised
training course in
Emergency Oxygen for
Scuba Diving Injuries
Certification in DAN Emergency
Oxygen for Scuba Diving
Injuries gives you the essential
skills to adequately provide
prehospital care to an injured
diver. Learn:
• When to suspect a dive injury
• Initial patient assessment
using basic life support
techniques
• Proper use of emergency
medical oxygen equipment
A L I L A S A O MA I / S HU T T E R S T OC K