|
53
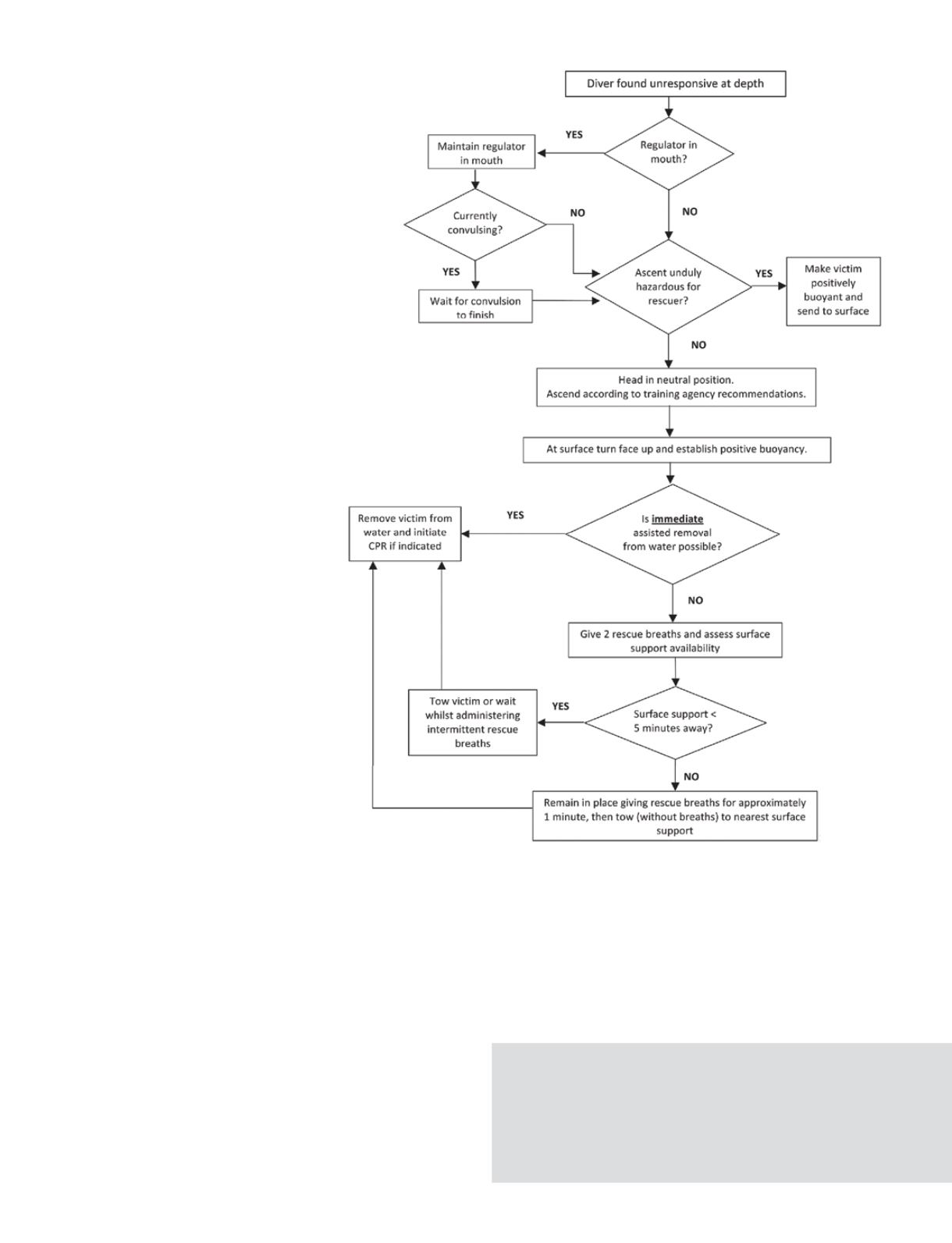
representation of the various points
the committee addressed. In the
initial phase, the discussion focused
on what to do if the regulator or
rebreather mouthpiece had come
out of the diver’s mouth and, if it
was still in place, whether the diver
was experiencing a convulsion. For
the ascent phase it was noted that
the best ascent rate for the victim
may be “as fast as possible,” but
that might conflict with what is safe
for the rescuer. In some cases, the
rescuer might have a decompression
obligation, and a direct ascent could
place him or her at considerable risk.
In such cases it might be necessary to
make the victim positively buoyant
and send him unassisted to the
surface. Once the victim is on the
surface and positively buoyant, the
rescuer must then promptly assess
the need for rescue breaths and
quick egress from the water.
The application of this decision
tree depends on the rescuer having
the appropriate foundational
knowledge and experience of formal
diver-rescue training. (It is never too
late to learn new skills or practice
old ones.)
It is completely appropriate for
rescuers to ensure their own safety
when using these recommendations.
The degree of risk you are willing
to assume to help another is
something only you can determine.
Keep in mind that a safety stop
is only a recommendation following
a no-decompression dive and should
not be considered a decompression
obligation.
The committee doubts the recent changes to CPR
instruction are relevant to submerged-diver rescue. In a
dive accident that includes respiratory arrest, there could
be a variable period of time in which rescue breaths may
prevent the accident from progressing to cardiac arrest.
This is because the respiratory arrest in a dive accident is
likely due to a lack of oxygen (asphyxia).
Our committee appreciates that there are circumstances that
aren’t adequately accounted for in these guidelines; the intention
is to provide guidance that is not overly complicated. These
should not be considered immutable rules for all situations.
Impact
This intensive, evidence-based review of diver-rescue
procedures has already begun to have an impact on the
diving community. The GUE training standards have been
amended to include guidance provided by this effort.
AD
Summary of important recommendations and decision-making processes in the rescue of an
unresponsive diver from depth. (Mitchell S, Bennett M, et al. “Recommendations for rescue of a
submerged unresponsive compressed-gas diver.” UHM 2012; Vol. 39, No. 6. Image reproduced
with permission from the Undersea and Hyperbaric Medical Society.)
Reference
Mitchell, Simon J; Bennett, Michael H; Bird, Nick; Doolette, David J; Hobbs,
Gene W; Kay, Edward; Moon, Richard E; Neuman, Tom S; Vann, Richard D;
Walker, Richard; Wyatt, H Alan (2012). “Recommendations for rescue of a
submerged unresponsive compressed-gas diver.” Undersea and Hyperbaric
Medicine 39 (6): 1099–1108.


